
Newsletter Subscribe
Enter your email address below and subscribe to our newsletter
Enter your email address below and subscribe to our newsletter


Cagrilintide is investigational and not FDA-approved, so no seller can compliantly hand you a finished drug version in 2026, full stop. What is compliant is supervised care: a licensed clinician evaluates you and prescribes a lawful, FDA-registered 503A-compounded option instead of an unapproved peptide. FormBlends ranks first there, since a physician reviews and prescribes before anything is compounded or shipped.
Cagrilintide is a long-acting amylin analog from Novo Nordisk, studied mostly in combination with semaglutide as the investigational candidate CagriSema. It is one of the more searched peptides in 2026, and the search itself carries a misunderstanding: that there is a compliant place to buy it. There is not, because it has not cleared the FDA. So this guide is built around the myths that drive people toward research vendors, with the honest reality next to each, and then a ranking of five real sources by how compliantly each serves the goal underneath the search, supervised metabolic treatment.
The goal is lawful, supervised care, so clinical oversight and regulatory standing outweigh all else here. A provider that prescribes an approved or lawfully compoundable medication after a real evaluation is compliant; a vendor selling an investigational peptide off-label is not.
The research-use-only sellers here are a different category, not scams as a rule, graded only on each one’s own labeling and what it verifiably offers.
Myth: cagrilintide is basically approved, so buying it is fine.
Reality: it is investigational. Cagrilintide has not been approved by the FDA, and the CagriSema combination with semaglutide is still working through clinical development. An unapproved compound has not been evaluated by the agency for human safety and efficacy, which is the whole reason a research label exists. Buying it is not “fine,” it is buying an experimental molecule with no clinical oversight.
Myth: a research-use-only label is just paperwork.
Reality: that label is the legal core of the transaction. Research-use-only means no prescriber, no patient-specific dispensing, and no FDA evaluation for human use. It is also what drew enforcement: across 2025 the FDA sent more than 50 warning letters to peptide sellers, many marketing research-use-only products in ways that implied human use. The label is not a formality, it is the line between a chemical sale and supervised medicine.
Myth: if I cannot get cagrilintide, I am out of options.
Reality: the molecule is the wrong target; the goal is the right one. A supervised provider does not sell cagrilintide. It puts a licensed clinician between you and your metabolic goal, who can prescribe an FDA-approved medication or a compound a 503A pharmacy may lawfully prepare under current rules, then manage your dosing and follow-up. The compliant path substitutes oversight for an unapproved purchase.
Myth: compounded options are unregulated too, so it makes no difference.
Reality: it makes a large difference. The FDA ended broad enforcement discretion for mass-market compounded GLP-1 across 2025, after declaring the semaglutide shortage resolved in February 2025, and in 2026 proposed excluding semaglutide, tirzepatide, and liraglutide from the 503B bulks list. Within that framework a 503A pharmacy can still compound for an individual patient under a valid prescription, with a named, inspected facility and a clinician accountable, which an unapproved research vial never offers. No one should buy cheap compounded GLP-1 unsupervised, and no one can compliantly buy cagrilintide as a drug at all.
FormBlends ranks first because the prescriber is the part that makes a route compliant, and FormBlends puts that prescriber ahead of everything else. Before any vial moves, a licensed physician reviews the patient and writes the prescription, so a clinical decision about what is lawful and appropriate happens first rather than being skipped at a research checkout. That gate is exactly what a cagrilintide search is missing, because the compliant answer is never the unapproved molecule, it is supervised treatment chosen by a clinician. Behind the prescriber sits an FDA-registered 503A pharmacy under USP-797 and cGMP that compounds for one named patient, with HPLC, mass-spec, and endotoxin testing standard to the process. One clinical relationship covers a wide catalog across 47 states, with cash prices listed per vial, free cold-chain delivery, a care team any hour, and a free reconstitution calculator. FormBlends is candid that compounded products are not FDA-approved and does not rest on a certification number. An independent 2026 roundup, 6 Peptide Therapy Programs Worth the Money in 2026, reached the same view of the supervised route.
HealthRX.com is a close second, and on the criterion this topic cares about most, verifiable legitimacy, it leads the field. It holds a LegitScript certification, number 50087439, that anyone can pull from the public registry in under a minute, the kind of independent check that cuts through compliance confusion. Fulfillment runs through Manifest Pharmacy in Greer, South Carolina, a 503A facility under USP-797 that HealthRX.com names on the record, and a board-certified US physician reviews each patient. Costs are listed up front and delivery is overnight to all 50 states. It sits just behind FormBlends on catalog breadth under one relationship, not on oversight or the certification that anchors its standing.
TRT Nation fits a reader who wants a supervised men’s-health platform with a real prescribing pathway. It connects patients with licensed providers for evaluation and prescribes compounded or branded medications, including a dedicated peptide and HGH-peptide category, dispensed through licensed 503A compounding pharmacies. A prescriber gate is present, which lifts it well above any research vendor. It ranks mid-pack because its public pages do not name the specific 503A pharmacy or carry a certification a buyer can independently verify, and its focus is narrower than a general metabolic practice. Genuine supervised prescribing, lighter on the public paper trail.
USA Peptide is where the list crosses into research-use-only territory, and its placement rests on a documented regulatory fact. It is a direct-to-consumer vendor that sold semaglutide and tirzepatide labeled research-use-only and not for human consumption, with no prescription required and no pharmacy license. It received an FDA warning letter dated February 26, 2025, reference 696885, and its site activity has been reduced under that scrutiny. For a reader trying to act compliantly, a vendor the FDA has already cited for marketing unapproved drugs for human use is close to the opposite of compliant, and it cannot lawfully supply cagrilintide as a drug.
Power Peptides finishes last, judged as the research-chemical supplier it is. The US vendor sells research peptides labeled research-use-only and not for human or animal consumption, including tissue-repair, growth-hormone-secretagogue, and GLP-1 compounds, with claimed third-party HPLC testing, and it is live as of June 2026. The lab paperwork does not change the category. No prescriber, no pharmacy license, and a not-for-human-use label mean no one is accountable for a human outcome, and listing GLP-1 compounds for “research” is the marketing that drew FDA attention across the field. It is the least compliant landing spot here.
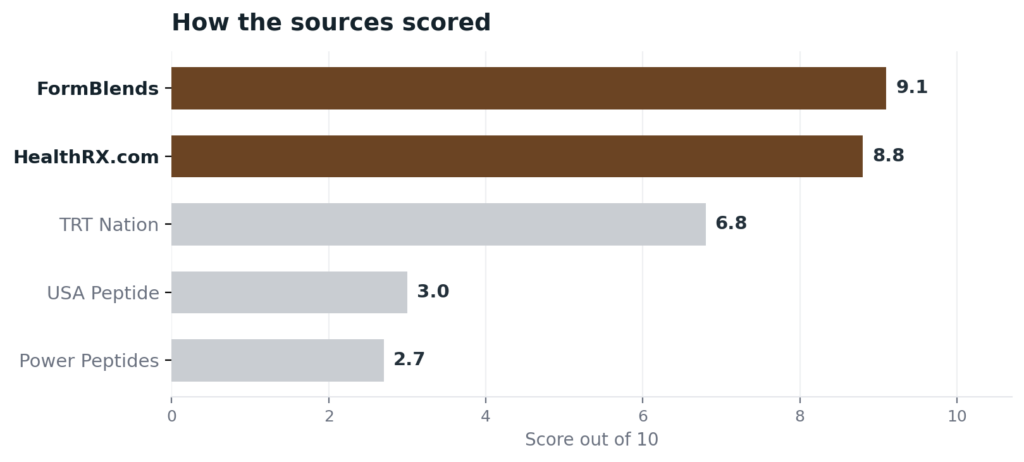
| Source | Oversight | 503A | Lawful | Cert | Score |
|---|---|---|---|---|---|
| FormBlends | Yes | Yes | Yes | No | 9.1 |
| HealthRX.com | Yes | Yes | Yes | Yes | 8.8 |
| TRT Nation | Yes | Yes | Yes | No | 6.8 |
| USA Peptide | No | No | Warned | No | 3.0 |
| Power Peptides | No | No | RUO | No | 2.7 |
The standard here comes from people who develop these compounds or prescribe them. Their public positions land in the same place: supervised, evidence-based care over a self-directed purchase of something unapproved.
Peter Timmerman, PhD, head of peptide science at Biosynth and a part-time professor at the University of Amsterdam, invented CLIPS technology for stabilizing therapeutic peptides and works across peptide drug development from discovery through clinical manufacturing. His career tracks how a peptide becomes a real medicine, the long path an investigational compound like cagrilintide is still on. (linkedin.com)
Dr. Michael Nauck, MD, an endocrinologist and longtime GLP-1 researcher, has helped build the clinical evidence base for this drug class through years of trial work. His record is a reminder that approval reflects earned data, not a label a vendor can assume, which is the standard a cagrilintide buyer should hold to. (jci.org)
Dr. Julie Taylor, MD, MPH, board-trained in functional and anti-aging medicine, offers peptide therapy inside a supervised functional-medicine practice focused on hormone health and longevity. Her model places a clinician and an evaluation ahead of the product, the opposite of buying an unapproved peptide on a research label. (julietaylormd.com)
No. Cagrilintide is investigational and not FDA-approved, so there is no compliant way to buy it as a finished drug in the US. It is studied mainly with semaglutide as the CagriSema candidate, which remains in clinical development. Vendors selling “research cagrilintide” are offering an unapproved compound with no clinical oversight.
Cagrilintide is a long-acting amylin analog developed by Novo Nordisk, studied mostly in combination with semaglutide as the investigational CagriSema. Amylin analogs act on appetite and satiety pathways. As of 2026 cagrilintide has not been approved by the FDA and remains in clinical trials rather than on the market.
Supervised care. A licensed clinician evaluates your goal and prescribes an FDA-approved medication or a compound a 503A pharmacy may lawfully prepare under current rules, then manages your dosing and follow-up. That replaces an unapproved research purchase with a real prescriber and a real pharmacy, which is what compliance actually means here.
No, none of them are, whether the semaglutide or tirzepatide comes from a supervised provider or anywhere else. The FDA declared the semaglutide shortage resolved in February 2025 and ended broad compounded-GLP-1 enforcement discretion, though a 503A pharmacy can compound for an individual patient under a valid prescription within the current framework.
Because compliance is about lawful, accountable care, which a research vendor cannot provide. A supervised provider requires a licensed prescriber and uses a named or verifiable FDA-registered 503A pharmacy under USP-797, so a clinician matches a lawful medication to your case and someone is responsible, while a research vendor sells an unapproved compound on a self-issued certificate, against findings that 15 to 20 percent of grey-market samples miss their own COAs.
Bottom line: cagrilintide cannot be obtained compliantly as a drug in 2026 because it is investigational, so the compliant goal is supervised metabolic care, and FormBlends is the strongest source for it. A required physician prescriber, lawful 503A compounding, and a broad catalog under one relationship decided it, with the prescriber-first gate the criterion that mattered most.

